Dry eye, MGD, drops, treatment, TFOS DEWS III, West Yorkshire, Cleckheaton, IPL, LLLT, environment, lifestyle
Why Your Eye Drops Aren't Working — and What's Actually Going On
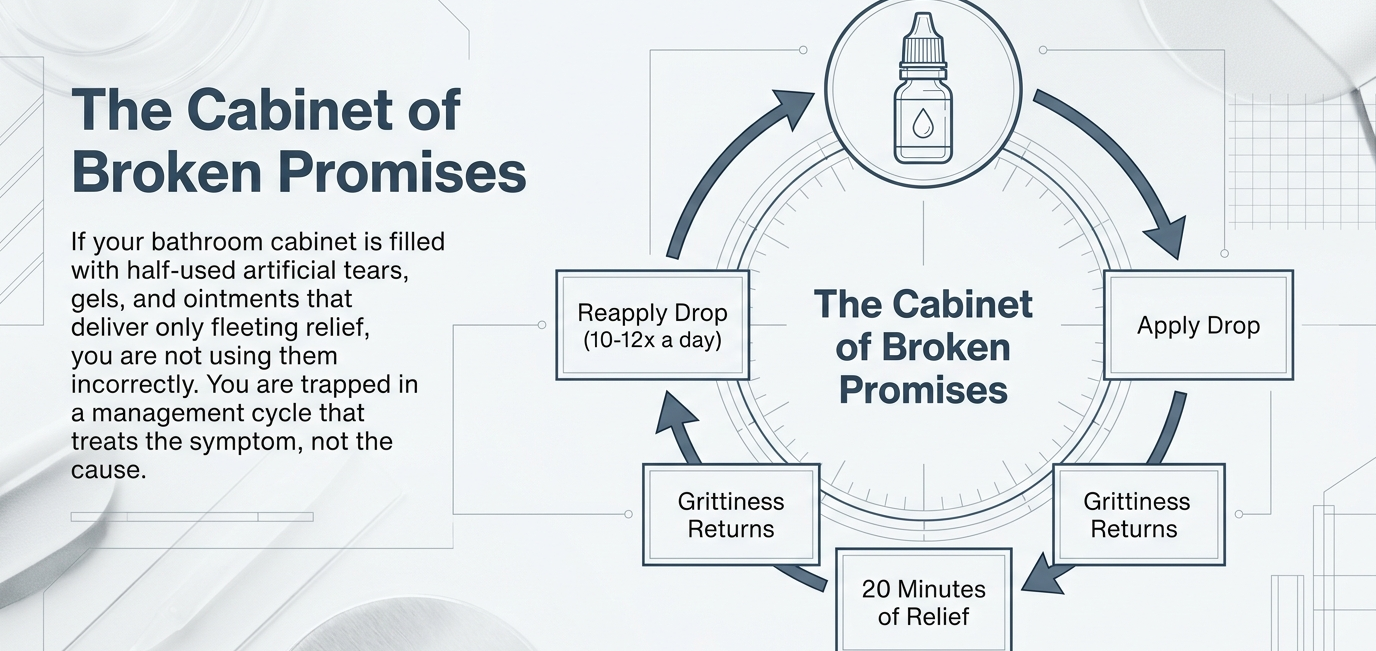
If you suffer from chronic dry eye, you probably own what one researcher memorably called a "cabinet of broken promises" — a collection of half-used bottles of artificial tears, gels, and ointments that each offered hope and delivered only minutes of relief.
You apply the drops. The grittiness eases. Twenty minutes later it's back. You apply them again. The cycle repeats, day after day, sometimes ten or twelve times a day, and nothing fundamentally changes.
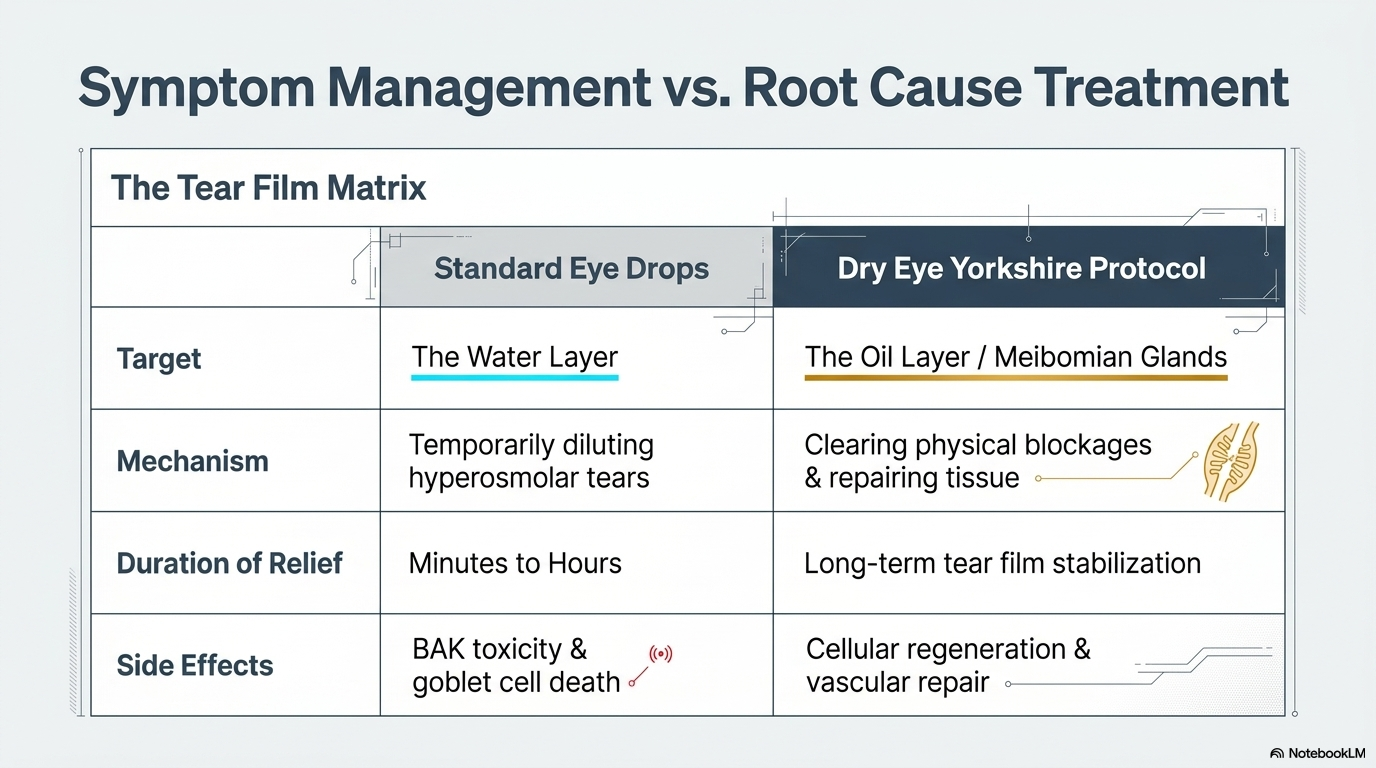
This is not because you're using the drops incorrectly. It's because drops are designed to manage a symptom — temporary dryness — not to treat the condition causing it. And for approximately 86% of people with chronic dry eye, the condition causing it has nothing to do with how much water their eyes are producing.
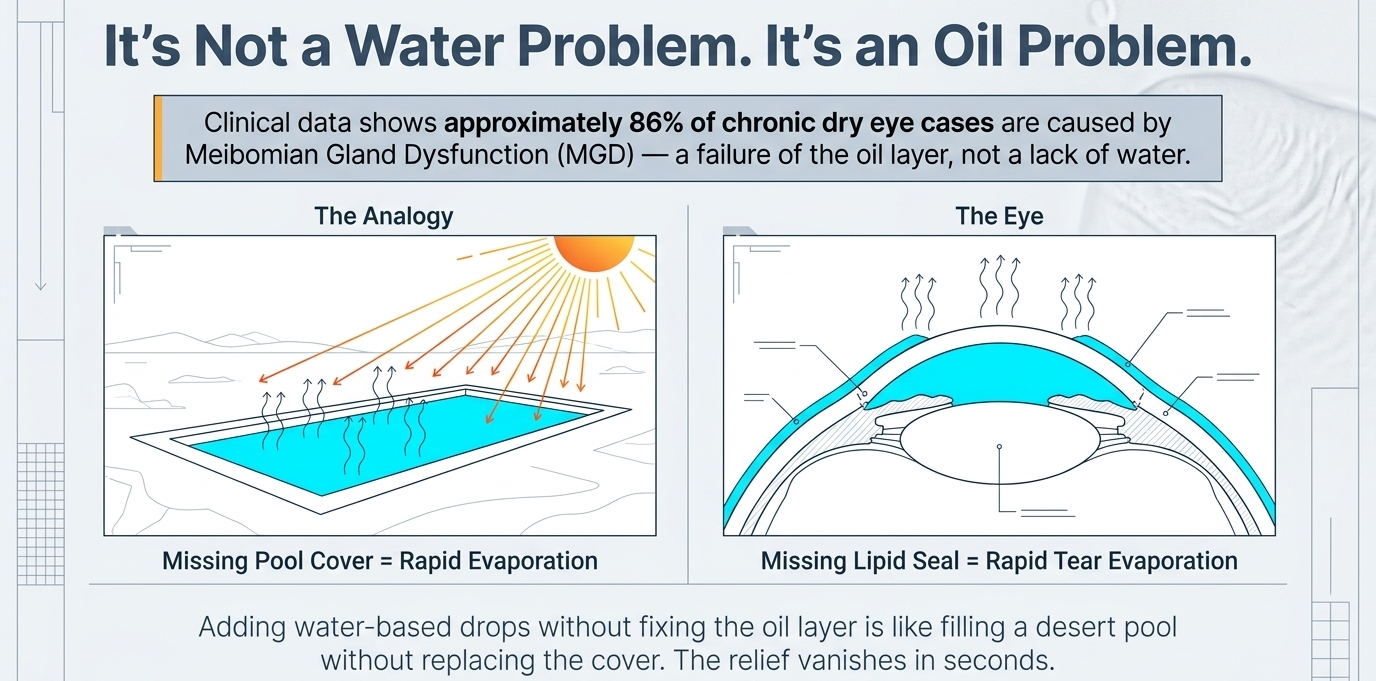
IT'S NOT A WATER PROBLEM. IT'S AN OIL PROBLEM.
Most people assume their eyes are dry because they aren't producing enough tears. This is understandable — it's the obvious inference from the sensation. But clinical data tells a different story. Around 86% of dry eye cases are caused by meibomian gland dysfunction — a problem with the oil layer of the tear film, not the water layer.
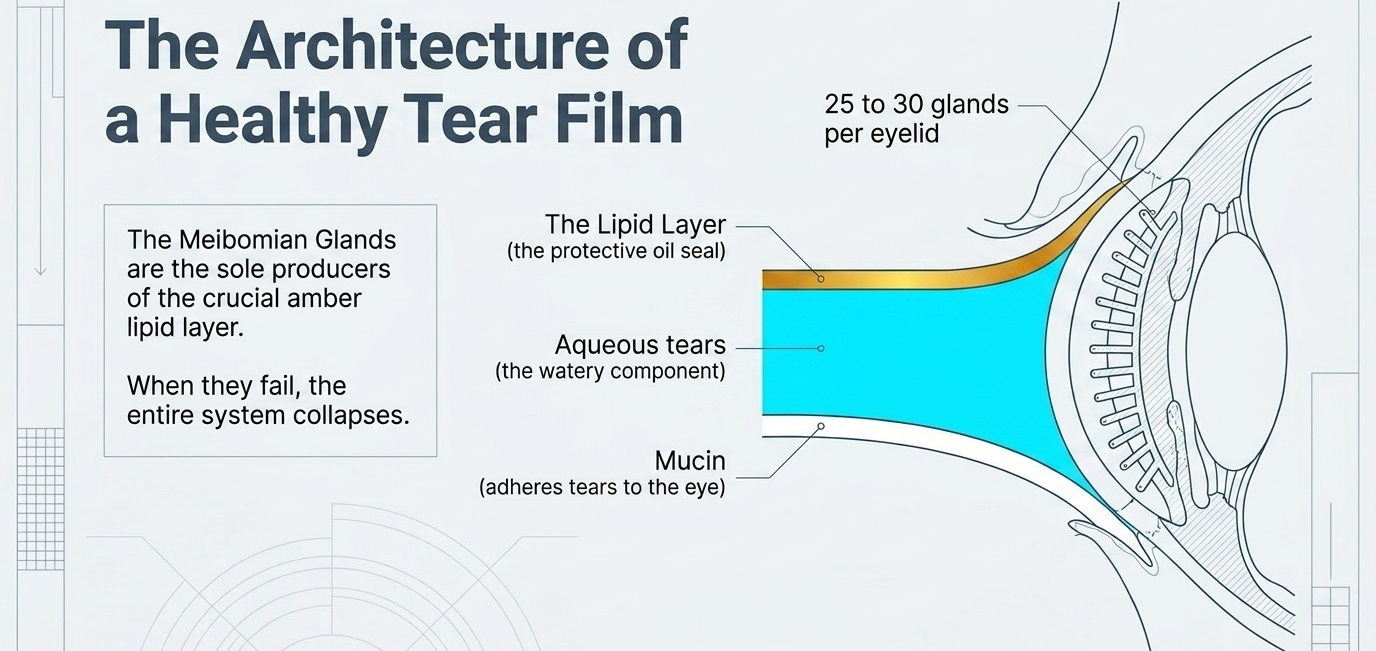
Your tear film has three layers. The innermost is mucin, a gel that helps tears adhere to the eye surface. The middle layer is the watery component — aqueous tears, the part that drops supplement. The outermost layer is oil, produced by the meibomian glands inside your eyelids.
That oil layer has one essential job: it acts as a seal across the surface of your tears and stops the water underneath evaporating.
Think of it like a swimming pool in the middle of a desert. If the water level keeps dropping, the problem usually isn't a leak in the floor — it's the absence of a cover. Without a cover, the sun and wind steal the water almost instantly. The same principle applies to your tear film. Without a healthy oil layer, your tears evaporate in seconds rather than the minutes they should. The eye surface dries out. Inflammation follows. The discomfort cycle begins.
Reaching for a water-based drop when your oil layer is missing is the equivalent of adding more water to the pool without ever replacing the cover. The relief is fleeting because the underlying problem — the missing seal — remains entirely unaddressed.
Tagline
YOUR ENVIRONMENT MAY BE WORKING AGAINST YOU
Before we look at what's happening in your glands, it's worth considering what's happening around them — because for many patients, their daily environment is actively undermining their tear film faster than any treatment can restore it.
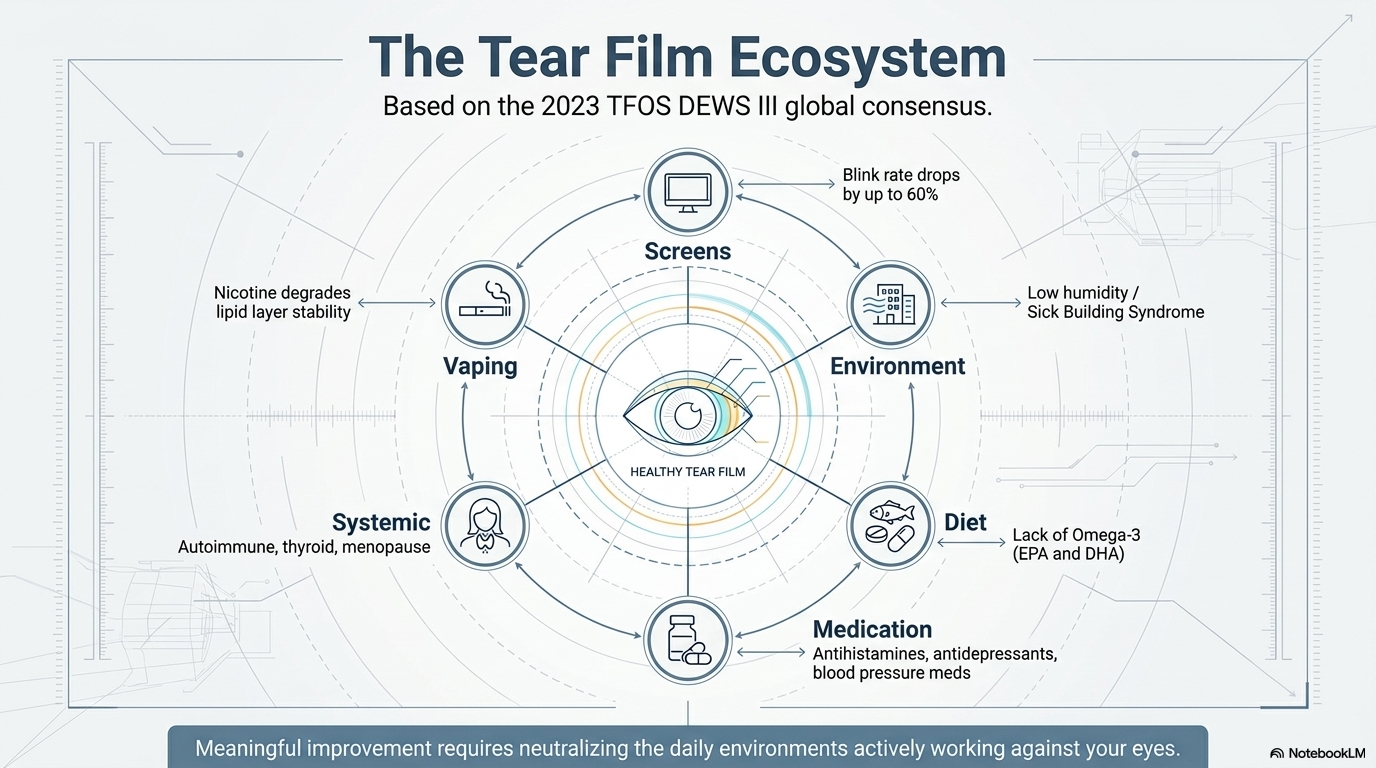
The TFOS DEWS III — the most comprehensive global consensus on dry eye, updated in 2023 by the Tear Film and Ocular Surface Society and involving hundreds of international researchers across multiple disciplines — specifically expanded its guidance on the environmental and lifestyle drivers of dry eye disease. The message is clear: treating dry eye effectively means looking at the whole picture, not just the eye in isolation.
The factors we routinely explore with patients include:
Screen time and blink rate. When we concentrate on a screen, our blink rate drops by up to 60%. Incomplete and infrequent blinks mean the meibomian glands aren't being stimulated to express oil, and the tear film isn't being refreshed across the eye surface. If you spend most of your working day in front of a screen, this alone is a significant driver of symptoms — regardless of what else is going on.
Indoor environment. Heated and air-conditioned spaces dramatically reduce ambient humidity. Low humidity accelerates tear film evaporation even in eyes with normal gland function. What researchers have termed "Sick Building Syndrome" — where symptoms are consistently worse in certain office or home environments — is a recognised clinical phenomenon. Identifying your environmental triggers is sometimes as impactful as clinical treatment.
Diet and nutrition. Omega-3 fatty acids play a documented role in meibomian gland health. The anti-inflammatory properties of omega-3s — particularly EPA and DHA — are supported by good evidence as an adjunct to dry eye management. We discuss diet and appropriate supplementation with every patient as part of a comprehensive plan.
Medications. Antihistamines, antidepressants, anxiolytics, isotretinoin, and certain blood pressure medications are all known to reduce tear production or stability. If you are taking any of these regularly, your medication may be a significant contributing factor to your symptoms — and it's worth discussing with us and with your prescriber.
Vaping. Evidence incorporated into DEWS III confirms that nicotine-containing e-cigarettes reduce tear film stability and damage the lipid layer, with worse effects at higher vaping voltage. This is a factor that many patients have not previously been asked about.
Systemic conditions. Autoimmune conditions, thyroid disease, rosacea, and hormonal changes — particularly menopause — all have documented connections to dry eye disease. A proper assessment considers your full medical history, not just your eye symptoms in isolation.
We raise all of this not to overwhelm, but because meaningful improvement in dry eye often requires changes in several areas simultaneously. In-clinic treatment works best when it is supported by an environment and lifestyle that isn't actively working against it. Part of what we do at your assessment is identify which of these factors are relevant to you specifically — and give you practical guidance on addressing them alongside any clinical treatment.
---
WHAT'S HAPPENING INSIDE YOUR EYELID GLANDS
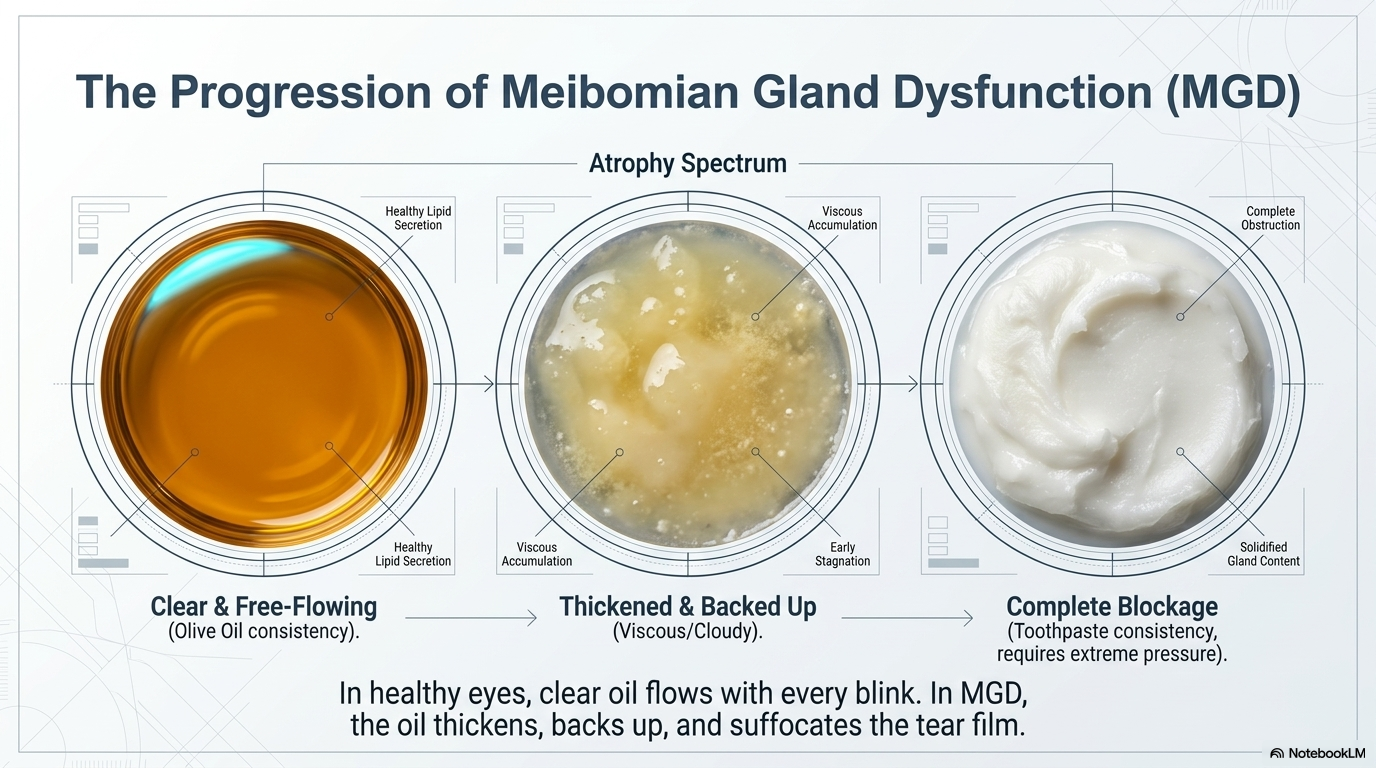
You have around 25 to 30 meibomian glands in each eyelid. In healthy glands, the oil they produce is clear and flows freely — almost like olive oil — with every blink. In meibomian gland dysfunction, that oil thickens and changes character. The gland openings become blocked. The oil backs up. What should flow freely becomes viscous and cloudy, and in more advanced cases toothpaste-like in consistency — thick, pale, and requiring significant pressure to express.
This is what we often see when we examine and express a patient's glands during a proper dry eye assessment. What comes out — or doesn't — tells us more about the state of someone's tear film than almost any other single test.
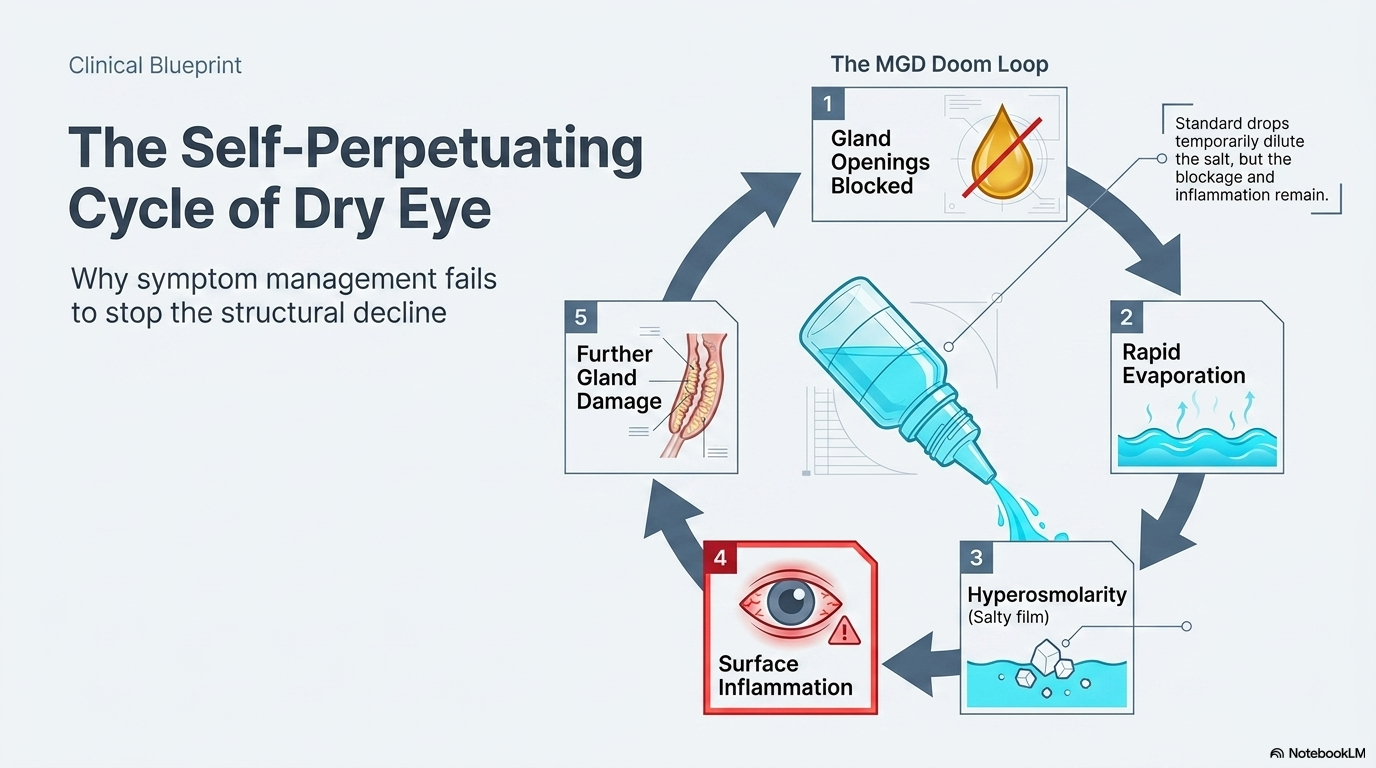
The consequence of chronically blocked glands is a self-perpetuating cycle. Without oil reaching the eye surface, tears evaporate too quickly. As the tear film becomes unstable, it becomes more concentrated — hyperosmolar — and that concentrated, salty film triggers inflammation on the eye surface. That inflammation further damages the gland openings and surrounding tissue. The glands become less functional. The oil supply diminishes further. The dryness worsens.
Standard drops break into this cycle briefly — they dilute the concentrated tear film for a moment and provide surface relief — but they do nothing to address the blockage, the inflammation, or the progressive gland dysfunction driving the whole process. The cycle restarts as soon as the drop evaporates.
A CRUEL IRONY — WHEN THE DROPS MAKE THINGS WORSE
There is a particularly uncomfortable reality for people who have been using drops heavily for a long time.
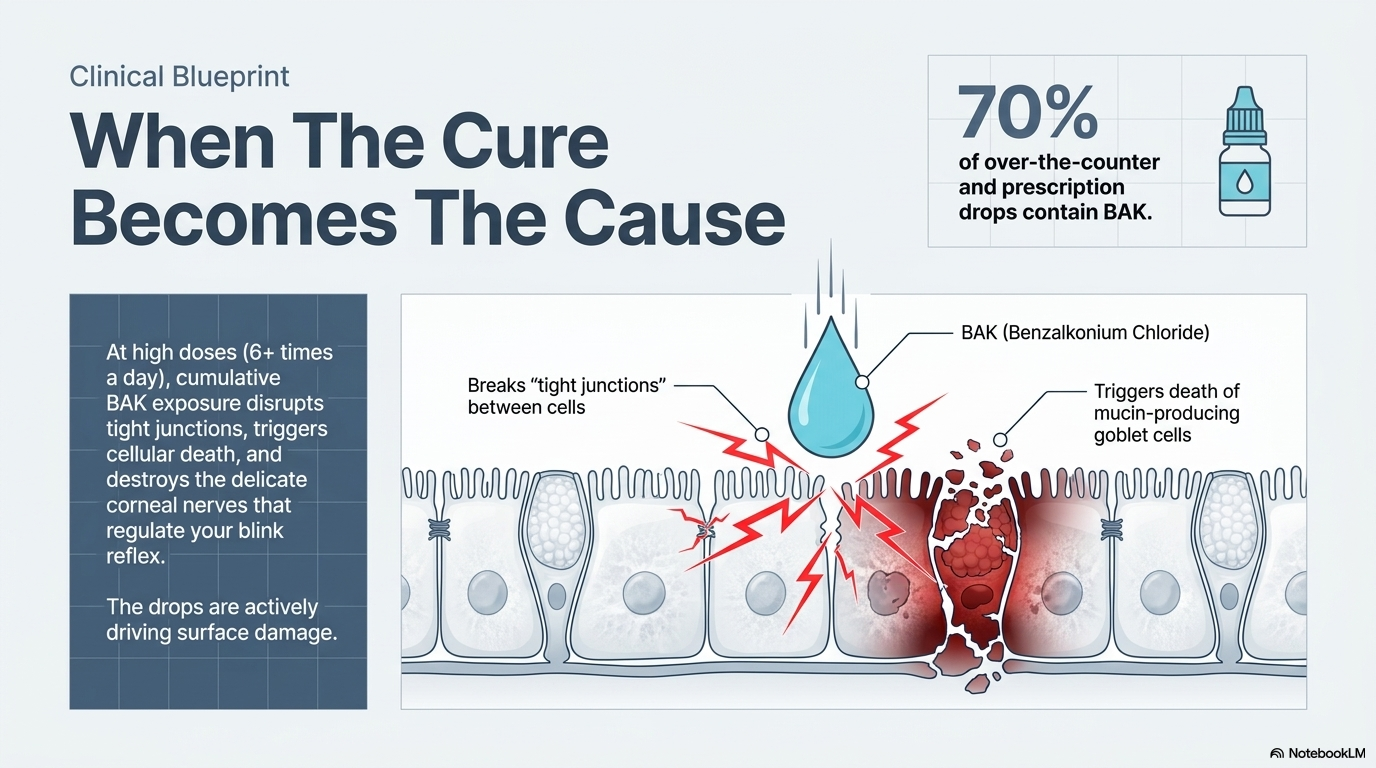
Some over-the-counter and prescription eye drops contain a preservative called benzalkonium chloride — BAK. For occasional users, this is largely irrelevant. But for someone using drops six, eight, or ten times a day, the cumulative exposure to BAK becomes clinically significant.
BAK is toxic to the ocular surface at repeated doses. It disrupts the tight junctions between the epithelial cells, causes programmed cell death, and destroys the goblet cells responsible for producing the mucin layer — the very inner layer that helps tears adhere to the eye surface. It also damages the delicate corneal nerves that regulate the blink reflex and tear production.
In other words: for the chronic dry eye sufferer, the very drops being used to manage the symptoms may be actively contributing to the surface damage driving them. The more drops you use, the more BAK exposure, and the more ocular surface disruption.
If you are using drops repeatedly throughout the day and your symptoms have been getting progressively worse rather than stable, this is worth knowing. Preservative-free formulations are significantly better tolerated and switching to these is often one of the first practical recommendations we make.
(Please use this information responsibly. Do not stop taking a medication that you have been prescribed without consulting your eye care provider. If you are concerned about BAK in a prescription medication, please ask your eye care provider if there are alternatives that will be equally effective.)
WHY YOUR EYES LOOK FINE BUT FEEL TERRIBLE
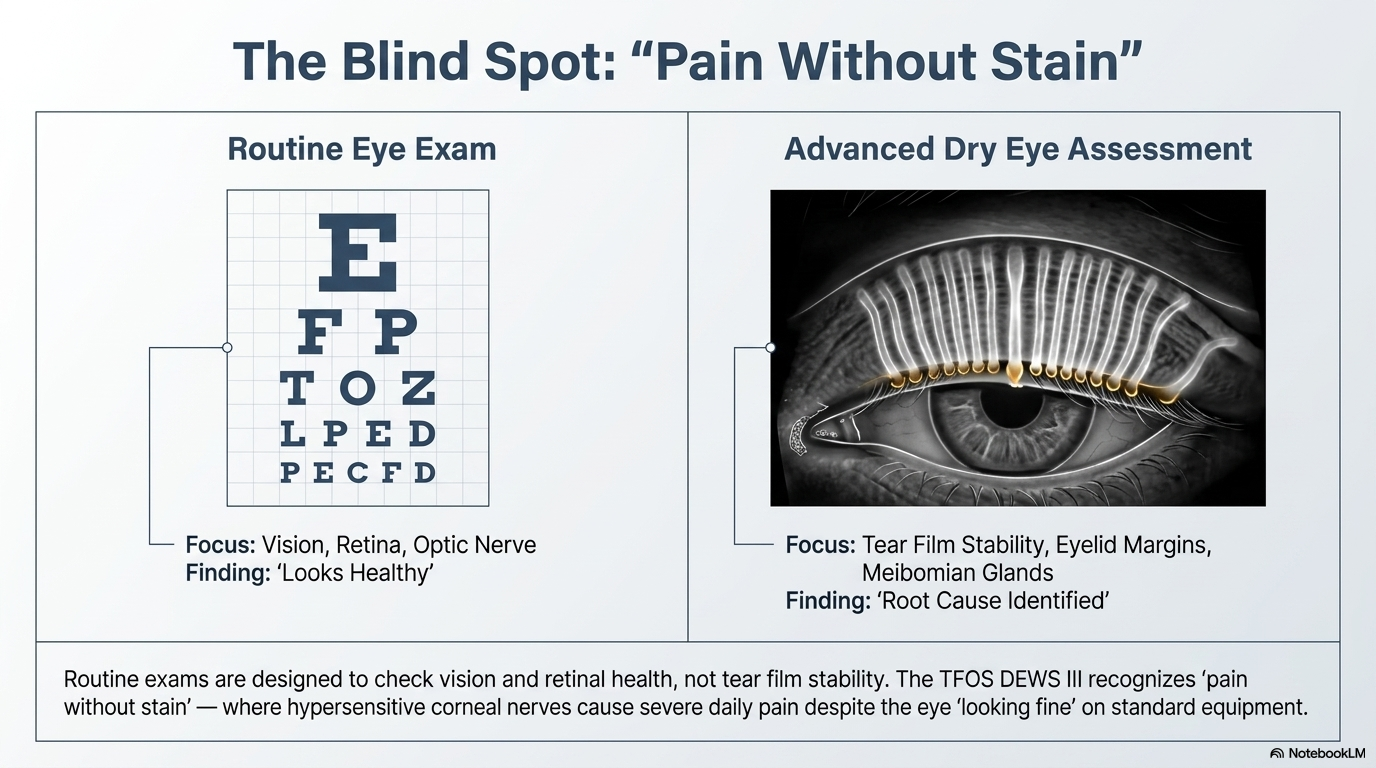
Many of the patients we see at Dry Eye Yorkshire have been told at a routine eye examination that their eyes look healthy. And in the terms a routine eye test is designed to assess — the structures of the eye, the retina, the optic nerve, the prescription — they are healthy. The routine examination was doing exactly what it is designed to do.
But a routine eye test is not designed to assess the meibomian glands, the tear film stability, or the eyelid margins. These are different clinical questions that require different equipment and a different examination protocol.
The TFOS DEWS III specifically recognises what is termed "pain without stain" — where a patient reports significant symptoms despite minimal visible signs at a standard examination. This reflects neurosensory changes in the ocular surface where the corneal nerves have become hypersensitive from chronic inflammation. It is a recognised clinical finding that validates the patient's experience. Being told your eyes look fine is not the same as being told nothing is wrong with your tear film.
If you have been told your eyes look fine but you are still experiencing daily symptoms, the right next step is an assessment that specifically looks at what a routine examination doesn't.
WHAT ACTUALLY TREATS THE CAUSE
The TFOS DEWS III is explicit that standard lubricating drops "do not target the underlying pathophysiology of dry eye disease." This is the scientific community's frank acknowledgement that drops are a management tool, not a treatment.
Treating the root cause of evaporative dry eye requires attention to the meibomian glands themselves. At Dry Eye Yorkshire, the treatments we use are:
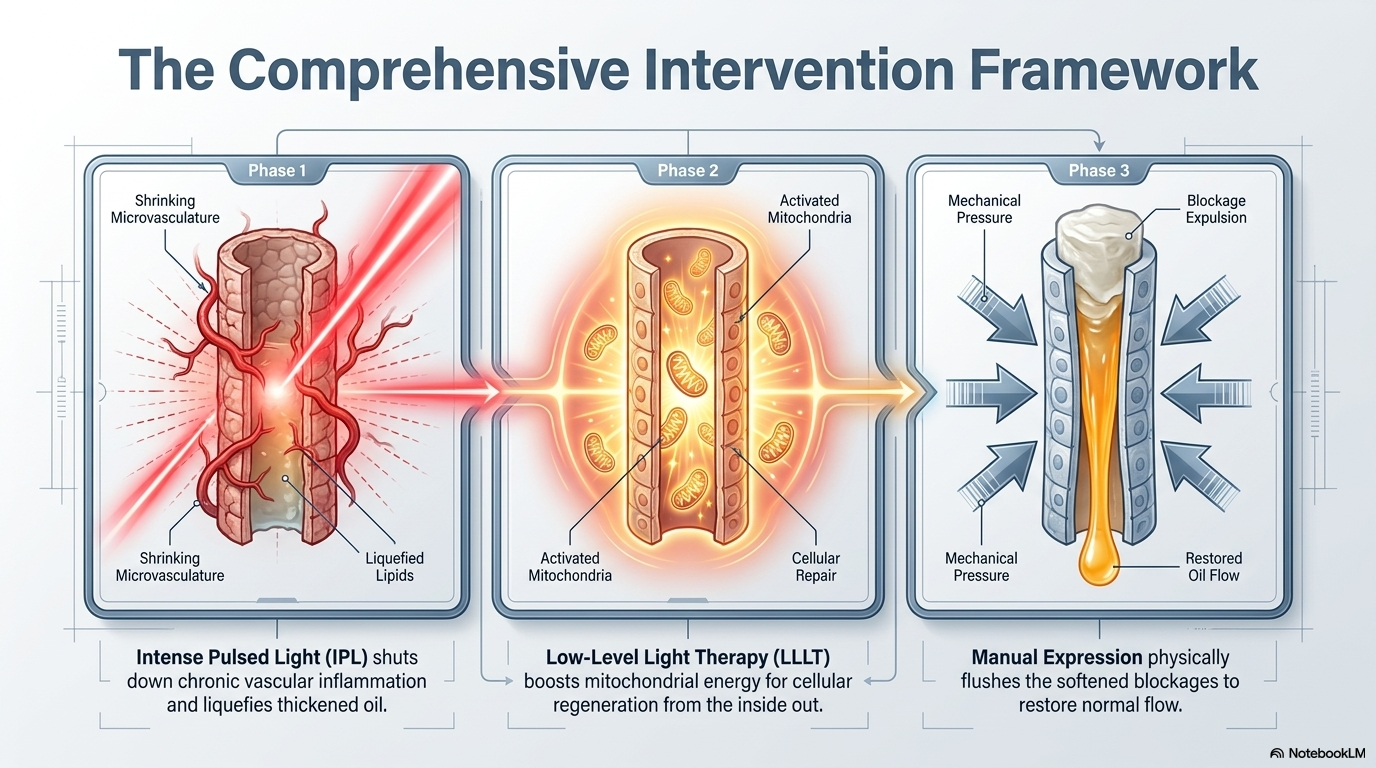
IPL — Intense Pulsed Light
IPL uses controlled pulses of light delivered to the periocular skin to address the chronic vascular inflammation driving meibomian gland dysfunction. The light energy targets the abnormal blood vessels along the eyelid margins — telangiectasia — that act as a reservoir for the inflammatory mediators degrading gland function. It also induces a thermal effect that liquefies thickened meibomian oil and stimulates cellular repair within the glands. Clinical trials consistently show significant improvement in tear stability and patient symptom scores. Our optometrist has undergone IPL treatment himself.
LLLT — Low-Level Light Therapy
Photobiomodulation therapy delivered through a mask placed over the closed eyelids. Red and near-infrared wavelengths stimulate the mitochondria within the eyelid cells, boosting cellular energy production and promoting tissue repair from the inside out — without external heat or conductive gel. We also use blue light LLLT, which targets the bacterial load and demodex activity at the lid margin. We combine LLLT with IPL for most patients. The two treatments are synergistic — IPL addresses the vascular inflammation and gland blockage while LLLT supports the cellular recovery of the glands themselves. Research shows the combination produces significantly greater improvement in symptoms than either treatment alone.
Meibomian gland expression
After every warming treatment, we manually express the meibomian glands to clear the softened oil. Warming the glands without expressing them is like heating a blocked pipe without flushing it — the softened material needs to be cleared to restore normal flow. We include manual gland expression as a standard part of every treatment session. This step is not universally offered and in our view it is essential to the effectiveness of any heat or light-based treatment.
WHY TIMING MATTERS
There is one important reason not to delay indefinitely.
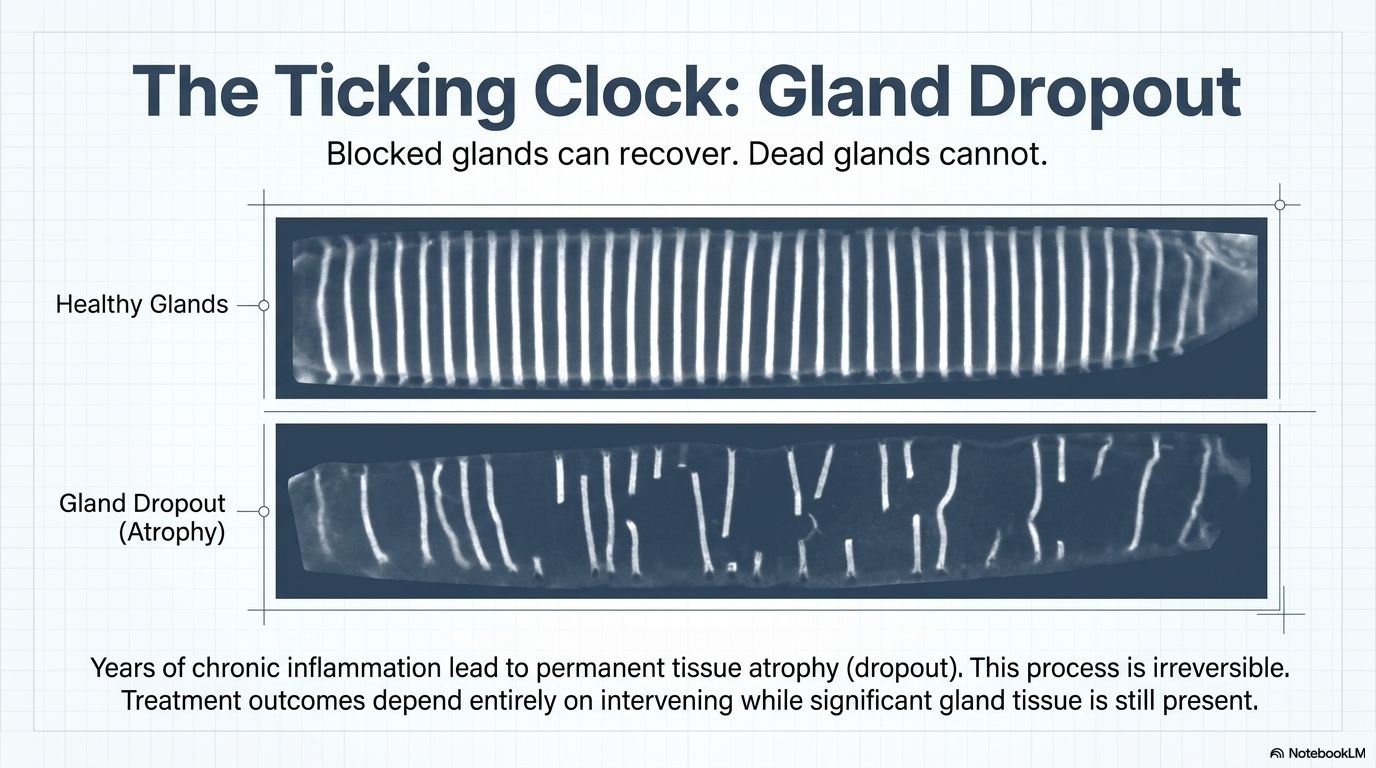
Meibomian glands that are blocked or underactive can recover function with appropriate treatment. But glands that have undergone atrophy — where the gland tissue itself has been permanently lost — cannot regenerate. The clinical term for this is gland dropout, and it is irreversible.
Dropout is a slow process, driven by years of chronic inflammation and the gradual atrophy of disused gland tissue. The longer MGD goes untreated, the more gland tissue is at risk. Treatment outcomes are consistently better when significant gland tissue is still present — even if underperforming — than in cases where substantial dropout has already occurred.
If you have been managing your dry eye with drops for months or years, some degree of this process may already have taken place. That is not a reason to panic. It is a reason to have a proper assessment now rather than continuing to manage with drops that are not addressing the cause.
WHAT A PROPER DRY EYE ASSESSMENT LOOKS LIKE
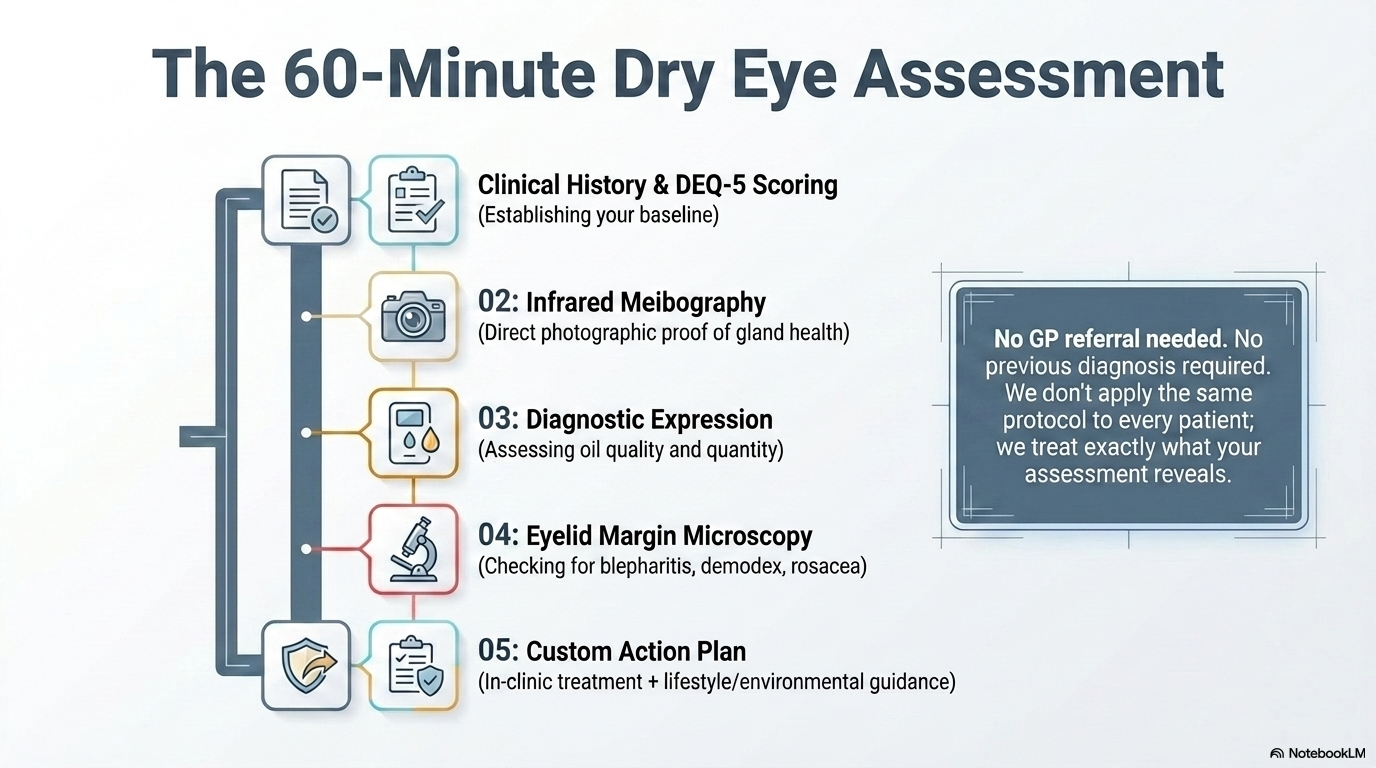
At Dry Eye Yorkshire, a dry eye assessment takes approximately 90 minutes. In that time we:
— Take a thorough clinical history including your symptoms, current treatments, medications, lifestyle, diet, and screen habits
— Score your symptoms using the DEQ-5, a validated dry eye questionnaire, giving us a baseline to measure your progress against
— Use infrared meibography to photograph your meibomian glands directly — showing us which glands are present, healthy, blocked, or lost
— Manually express your glands to assess the quality and quantity of meibomian secretion
— Examine your eyelid margins, lash line, and ocular surface under magnification for signs of blepharitis, demodex, rosacea, and inflammation
— Discuss the environmental, dietary, and lifestyle factors relevant to your specific presentation
At the end of the assessment, we tell you exactly what we found, what it means, and what we recommend — including both the in-clinic treatment options and the practical changes that will support them. We don't apply the same protocol to every patient. What you receive depends on what your assessment shows.
No GP referral is needed. No previous diagnosis is required.
IF YOU RECOGNISE THIS PICTURE
If you have been managing your dry eye with drops for months or years and still experience daily symptoms, there is very likely more that can be done. The drops are not failing because your dry eye is untreatable. They are failing because they are not treating the cause.
An assessment is the right starting point. It will tell you what is actually happening — in your glands, in your tear film, in your eyelid margins, and in the environment around your eyes — and what is most likely to help.
Dry Eye Yorkshire — Openshaw Opticians
Unit 4, 16 Cheapside, Cleckheaton, West Yorkshire, BD19 5AF
📞 01274 878214
We see patients from Cleckheaton, Heckmondwike, Liversedge, Mirfield, Batley, Dewsbury, Bradford, Halifax, Huddersfield, and across West Yorkshire.